SACRAMENTO (June 11, 2026) — The California Hospital Association is aligned with a broad coalition of health care organizations, unions, and everyday Californians in opposition to a ballot measure that would impose a tax on California’s wealthiest residents.
(more…)California Hospitals Oppose Billionaire Tax Ballot Measure
Provider Enrollment Information Available on Vaccines for Children Program
What’s happening: The California Department of Public Health (CDPH) has released provider enrollment information on the Vaccines for Children (VFC) Program.
(more…)Psychiatric Hospital Staffing Ratios Closing Beds Across CA, CHA News Release Warns
What’s happening: On Tuesday, CHA issued a news release describing how new staffing ratios for acute care psychiatric hospitals are forcing bed closures and driving youth and adults in mental health crisis into overcrowded emergency departments.
(more…)CHA-Sponsored Ballot Initiative Advances to November
Late last week, the CHA-sponsored initiative to give health care workers a voice in how their hard-earned dues money is spent on political campaigns qualified for the November 2026 ballot.
(more…)CHA Formally Opposes Billionaire Tax Act
What’s happening: Earlier today, CHA issued a news release aligning with a broad coalition of health care organizations, unions, and everyday Californians in opposition to a ballot measure that would impose a tax on the state’s wealthiest residents.
(more…)Applications Open for HCAI Behavioral Health Workforce Funding
What’s happening: Hospitals should consider applying for a new, multi-year $196 million behavioral health workforce recruitment and retention program recently launched by the Department of Health Care Access and Information (HCAI).
(more…)HCAI to Host Webinar on Planning for Disasters
What’s happening: The Department of Health Care Access and Information (HCAI) will host a webinar on July 7 from 10 to 11:30 a.m. (PT) that is focused on hospitals’ planning and preparing for disasters.
(more…)New Staffing Ratios Force Bed Closures and Drive Youth and Adults in Mental Health Crisis into Overcrowded Emergency Departments
SACRAMENTO (June 9, 2026) — Despite hospitals having hired more than 1,000 nurses to comply with new state staffing ratios at acute care psychiatric hospitals, an unworkable June 1 deadline has already resulted in fewer mental health services for Californians.
(more…)Fact Sheet: Medicaid in California
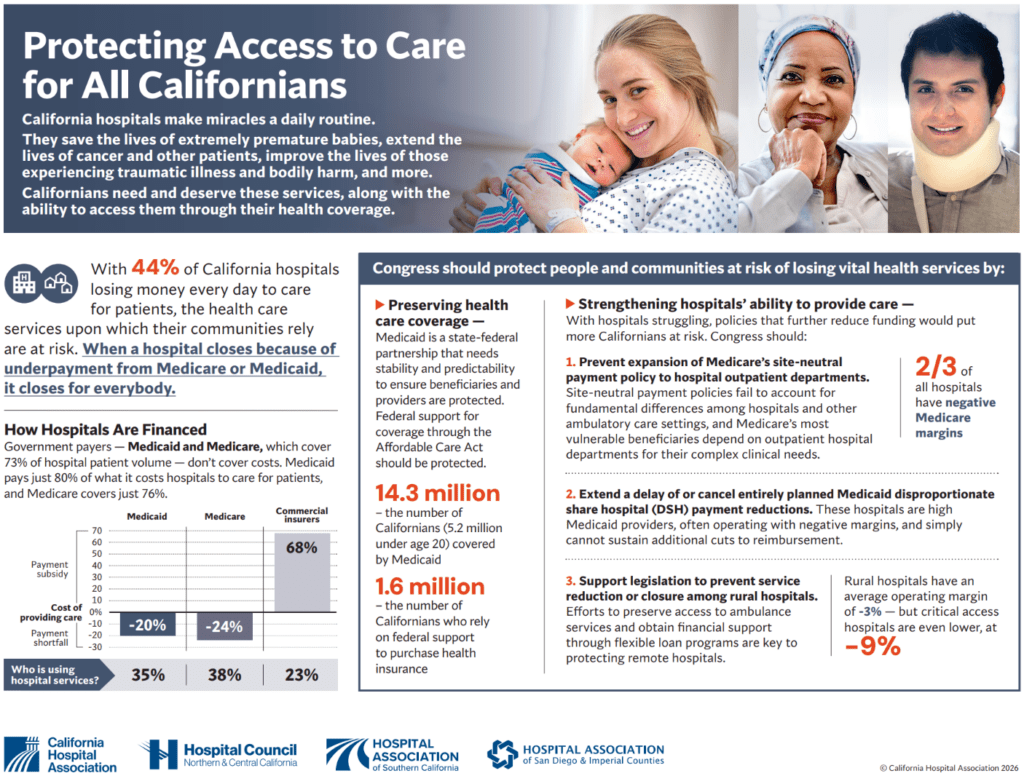
Infographic: Protecting Access to Care for All Californians